
Oral Health Care Screening in Pregnancy
DNP 711 Health Policy Blog by K. Flores
Arizona State University
Week Two 1/20-1/26: Oral Heath Care Screening in Pregnancy
Pregnancy is a unique health experience requiring an emphasis on preventative care to ensure healthy outcomes for mother and baby. Prenatal care visits are an opportunity to enhance patient education as well as evaluating for pregnancy development. However, oral health care during the antenatal period is an important health promotion aspect that is often neglected.
Early detection of periodontal disease in pregnancy may improve the oral health outcomes for mothers and infants. If left untreated, dental caries and bacteria acquired from pregnant mothers may be transmitted to infants and increase the risk for periodontal disease as children (Oral Health Care during Pregnancy Expert Workgroup, 2012). Absence of screening and treating dental disease during pregnancy may lead to preterm births, adverse birth outcomes, and an increased likelihood for poor oral health for mothers and infants (Children’s Dental Health Project [CDHP], 2018). In Arizona, the average costs related to care for premature births through the Arizona Health Care Cost Containment System (AHCCCS) ranges from $22,000 to $67,000 per year (MacDonal-Evoy, 2019).
The AZ Senate Bill 1088 provides coverage for dental screening and treatment for pregnant women through the AHCCCS (MacDonald-Evoy, 2019). The bill passed in the state senate in February 2019, granting Medicaid funding for comprehensive dental coverage for pregnant mothers at least 21 years old through their pregnancy and 6 months postpartum. Approval of SB 1088 enhances opportunity for oral health screening and treatment during pregnancy. However, there are still challenges for pregnant women to utilize these federal coverages and benefits.
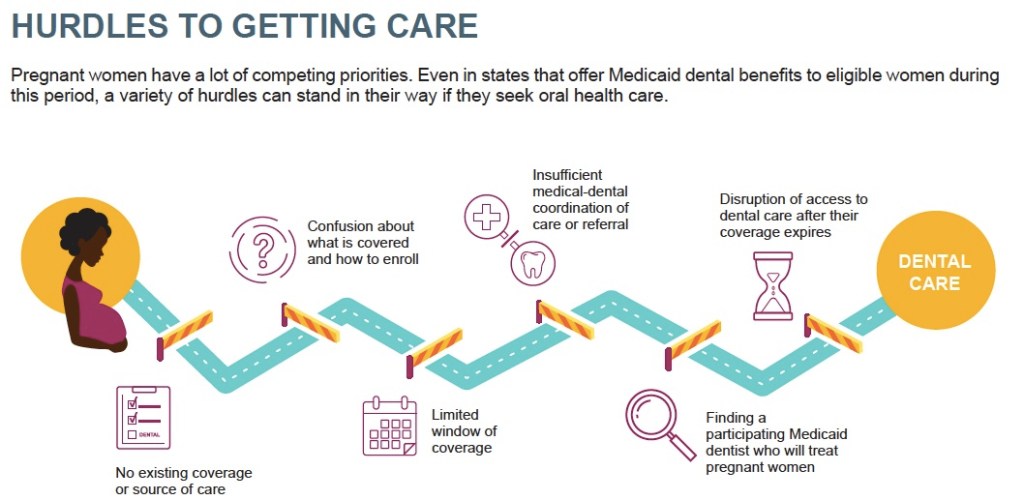
Many barriers exist in preventing women from receiving oral health screening in pregnancy: inadequate data representing coverage or access to care; inconsistent coverage from state to state; organizational, educational, and physical location barriers.
CDHP (2018)
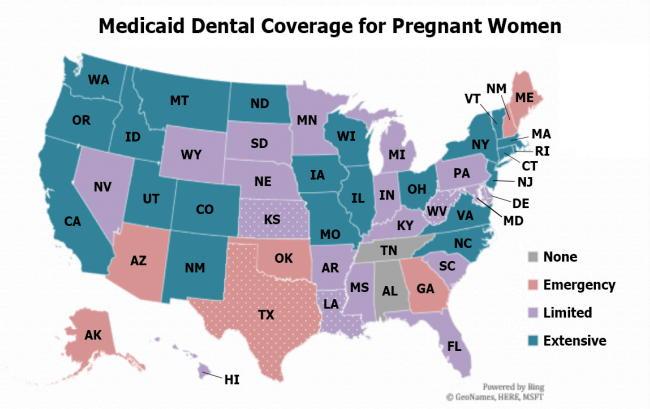
At the national level, oral health care screening in pregnancy is insufficient. Inadequate data for screening and access at the state and federal levels serves as a barrier to dental coverage for pregnant women (CDHP, 2018). Currently, data collection regarding oral health care during pregnancy is not recorded. Therefore, dental coverage is inconsistent from state to state and oral health care screening is thereby limited. Because a national standard for dental coverage in pregnancy does not exist, 40 states provide benefits up to 60 or 90 days postpartum, while other states do not provide any dental coverage for pregnant women (Eke, Mask, Reusch, Vishnevsky, & Quinonez, 2019).
A health policy solution that would increase oral health care screening during pregnancy may consist of uniform dental coverage during pregnancy among all 50 states extending until 1-year postpartum (Eke, Mask, Reusch, Vishnevsky, & Quinonez, 2019). This will aim towards standardized data among all states to evaluate access to oral health screening, treatment, and pregnant women’s health insurance benefits. Additionally, barriers which prevent pregnant women from accessing dental care such as, enrollment timing and eligibility windows may be alleviated.
Health policies are a driving force for change that produce effects at an individual and community level.
(Longest, 2010)
It is important to call attention to this health problem as both patients and providers do not place enough emphasis on oral health screening during pregnancy. While pregnant mothers may be unaware of the benefits of oral health screening, medical and dental providers often underutilize these screenings. As a future women’s health nurse practitioner, it is important to understand the significance oral health during pregnancy in order to provide comprehensive care to patients and promote optimal healthy behaviors during and after pregnancy.
References:
Children’s Dental Health Project. (2018, September). Oral health in pregnancy (Issue Brief No. 339). Retrieved from https://www.cdhp.org/resources/339-issue-brief-oral-health-during-pregnancy
Eke, C., Mask, A., Reusch, C., Vishnevsky, D., & Quinonez, R.B. (2019 November). Improving access to oral health care in pregnancy (Issue Brief No. 384). Retreived from https://www.cdhp.org/resources/384-coverage-brief-improving-access-to-oral-health-care-in-pregnancy
Longest, B.B. Jr. (2010). Health policymaking in the United States. (5th ed.). Chicago, IL: Health Administration Press.
MacDonal-Evoy, J. (2019). Carter proposes Arizona Health Care Cost Containment System (AHCCCS) dental coverage for pregnant women. Retrieved from https://www.azmirror.com/2019/01/23/carter-proposes-ahcccs-dental-coverage-for-pregnant-women/ Oral Health Care During Pregnancy Expert Workgroup. (2012).
Oral Health Care During Pregnancy Expert Workgroup. (2012). Oral Health Care During Pregnancy: A National Consensus Statement. Washington, DC: National Maternal and Child Oral Health Resource Center.

I am willing to submit that oral care was not previously at the top of my concerns list when evaluating a pregnant patient. As you mentioned, pregnancy affects every aspect of health, and it is likely that concern for other components takes precedent. I was initially surprised by the statement from the Oral Health Care During Pregnancy Workgroup (2012) that caries-causing bacteria in infants and young children may very well be transmitted from mother to child. Nevertheless, as I thought about my children/babies and I (admittedly not a mother), I can think of many ways bacteria could travel from one mouth to the other. Therefore, as a strong proponent of pediatric health promotion and disease prevention I applaud you and others for taking note of this issue and working towards a resolution. Beyond the obvious health benefits of achieving adequate dental coverage and care, there are financial benefits as well. An older study analyzed the financial benefits of preventative dental visits in the medicare population (Moeller, Chen, & Manski, (2010). They found that while the number of dental visits increased when medicare coverage was provided, costly non-preventative procedures were reduced. So, I believe this to be a pertinent issue for both the health and financial benefits it provides.
References
Moeller, J. F., Chen, H., & Manski, R. J. (2010). Investing in preventive dental care for the Medicare population: A preliminary analysis. American Journal of Public Health, 100(11), 2262-2269. doi: 10.2105/AJPH.2009.184747
Oral Health Care During Pregnancy Expert Workgroup. (2012). Oral health care during pregnancy: A national consensus statement [PDF file]. Retrieved from https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf
LikeLike
This information is so important for women’s health providers to be aware of. During clinical rotations, some NPs that I followed asked patients if they had been to the dentist in the last 6 months, but others did not. I wonder how aware providers are of this new bill and the referral process. Further, the fact that it can be difficult to find a dentist that not only accepts Medicaid patients, but will perform dental care on pregnant women makes this an even more difficult process.
Physiologic changes during pregnancy may result in noticeable changes in the oral cavity, such as dental caries, teeth erosion, tooth mobility, and pregnancy gingivitis. Providers such be aware of these changes and emphasize the importance of seeking dental care during pregnancy to recognize these changes before they worsen. Pregnancy is an optimal time to teach women, because they are motivated to adopt healthy behaviors for the wellbeing of their child (American College of Obstetricians and Gynecologists (ACOG), 2013). ACOG (2013) suggests women’s health providers address oral health at the first prenatal visit by asking these three simple questions:
1. Do you have swollen of bleeding gums, a toothache, problems eating or chewing food, or other problems in your mouth?
2. When was your last dental visit?
3. Do you need help finding a dentist?
I plan on incorporating this into my future practice but hope to learn the best way to answer the third question due to all the barriers that exist connecting these patients to who they need to see. I look forward to seeing how you address this issue in your blog and will continue reading your posts.
Reference
American College of Obstetricians and Gynecologists. (2013). ACOG committee opinion no. 569: Oral health care during pregnancy and through the lifespan. Obstetrics and Gynecology, 122, 417-22.
LikeLike